Here is my latest hearing test, any input would be most appreciated.
No problem.
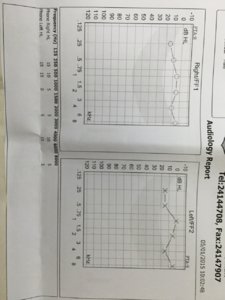
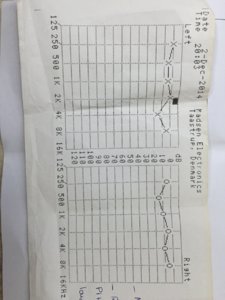
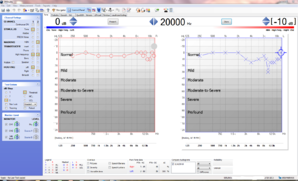
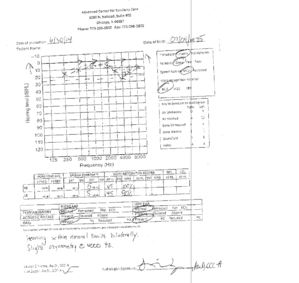
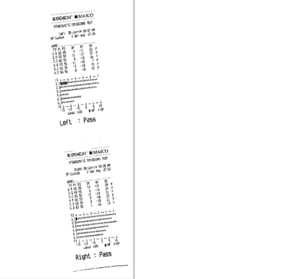
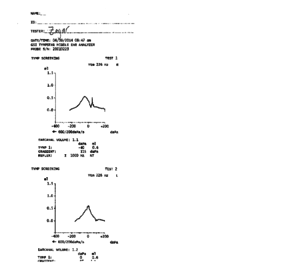
For your age (of about 40 years old), your hearing within the speech frequency range (0-8 kHz) is really quite good. You can in fact see the "speech banana" has been drawn (in a grey background colour) on this particular audiogram - and you are nowhere near entering that region. Additionally, you are within the "official limits" of showing no hearing loss i.e. hearing thresholds within 25db HL for a standard audiogram (0-8 kHz). In the very high frequency range (>8 kHz) you are showing a drop beyond that (especially right ear). However, there is relatively little literature on very high frequency audiology as the medical community has developed a practice of not testing it because there is no "need" from an audiology point-of-view (i.e. you don't need the higher frequencies above 8 kHz to detect speech, as you probably know). Furthermore, an audiogram cannot be used in order to detect tinnitus directly. But, based on literature from Dr. Wilden - who has refined the concepts of audiology for tinnitus purposes - early symptoms of cochlear overstrain start already with a hearing loss of 10db (or more). I had four consultations with Dr. Wilden (each lasted about 30 to 45 minutes), and I also had follow-up conversations via e-mail and telephone and I have also spent many hours of reading his online material, and based on that, I have no doubt that someone such as Dr. Wilden would say that your tinnitus is due to hearing loss in the higher frequency regions. Your hearing loss is asymmetrical (left/right ear) which provides a further clue (e.g. a unilateral ear infection, ototoxicity from topical ear medication, auditory insult from a single source of noise, etc.). The hearing test did not include the 0,125 kHz frequency; the 3 kHz frequency
was included; a bone-conduction test does not appear to have been carried out. That is what I see.
From my own personally acquired knowledge, there does not necessarily have to be a correlation between tinnitus severity and the extent of HL. In other words, it is perfectly possible for your complaint of "severe bothersome tinnitus" to be true both subjectively (and objectively!). Another "proof" of this is all the people who attend concerts and end up with tinnitus after the event. In many such cases the hearing threshold returns to normal levels some 24 to 48 hours after the auditory insult, but the tinnitus remains (and in some cases is severe regardless of audiometry findings which typically would be what they were before the incident).
It is difficult for me to "recommend" any remedial approach really. The conventional medical community (i.e. your average family physician, ENT, or neurologist) does not address subjective tinnitus diagnostically nor are they in a position to treat it (they don't have the competence/knowledge to do so as we are all aware). If you approach doctors who work within niche fields of medicine (e.g. Prof. Jeanmonod in Switzerland or ENT surgeons at the Acquaklinik in Germany) they will have a more refined understanding of tinnitus within their fields of study. A pre-consultation via telephone with Prof. Jeanmonod (neurosurgeon) would typically take some 15-20 minutes and based on your audiogram he would probably conclude that you do have
a loss of auditory input to the brain - which is the primary objective he tries to ascertain before being willing to accept you as a patient at his clinic (other criteria is that you have had the condition for a year or more and that you have made attempts to somehow rectify your situation via other means e.g. TRT, CBT, and/or off-label drugs). The patient review starts off with a high resolution EEG-scan which looks for a clinical finding of thalamocortical dysrhythmia (a concrete and objective diagnosis). Regardless of the exact findings, however, most patients will probably receive the diagnosis: chronic and resistant tinnitus. An ENT surgeon, on the other hand, and with knowledge of the latest developments in otology medicine would approach the situation using a mixture of objective findings along with a narrative diagnosis (i.e. letting you the patient tell the doctor what transpired prior to you - the patient - developing tinnitus). If there is sufficient evidence to suggest that you would qualify for an intervention using drugs such AM-101 or OTO-311, that could then theoretically proceed. The only problem is that the pharmas are currently not willing to supply doctors with their drugs for non-study purposes (I have previously attempted it via "official channels" i.e. a physician licensed to partake in clinical trials, and the answer from the pharmas was "no" even though the surgeon was willing to perform the procedure).
The above highlights the two main areas whereby the practical arm of medicine (as opposed to the theoretical arm) is attempting to treat patients medically: the neuro-perspective (loss of auditory input causing dysfunction(s) in the brain) and the cochlear-perspective (associated with certain pathology states of the inner ear, see literature on NMDA receptors, for instance). The AM-101 trial is aimed at acute tinnitus. The OTO-311 trial which is expected to go ahead later this year and does not yet a have a patient eligibility profile defined - at least not the last time I was in contact with Otonomy Inc (04/FEB/2015). But it is perhaps possible that they will accept patients with a longer history of tinnitus. I am also aware that Gacyclidine (OTO-311) is considered a more potent NMDA-antagonist than Esketamine (AM-101). AM-102 is of course another development which may be coming forward later on, but may only accept healthy volunteers to begin (and all of this is purely speculative on my part - and hence my use of "may").
Recently, there was a medical finding in relation to a single patient study of tinnitus which showed that tinnitus is "all over the brain" (or words to that effect). If I recall correctly, the article either concluded (or at least insinuated) that tinnitus may therefore be harder to treat (than previously thought). I am sure there are fine researchers behind the study, but I should like to just add a piece of "practical advice" in relation to such conclusions: all of the current neuro-physical models of tinnitus almost certainly assume that loss of auditory input is maintained (as conventional medicine has not yet figured out how to restore hearing loss). It is therefore "too easy" to conclude that tinnitus is more complex (and thereby insinuating that it is also more complex to treat) as we don't really know what happens if you were to restore auditory input (to the brain). Would the brain start show signs of plasticity and move away from its fixed pathological state if such a restoration were to take place? As I type these lines, I can say that my own tinnitus is a good 50% better than it was at the onset of my ordeal back in April, 2013. Back then, my tinnitus was "off-the-chart" especially at night-time with some 6-to-7 different tones when lying in horizontal position. Not so now. Not at all, in fact. I haven't used sleep medication (of any kind) since many, many months and I still fall asleep within a couple of minutes every night. Quite different from the early stages of my tinnitus ordeal when I would get perhaps 3 or 4 hours of seriously interrupted sleep per night. I did stem cell therapy and LLLT as well as several brief rounds of Flupirtine (in order to mitigate the risks of liver toxicity), and I have also been very disciplined with respect to using earplugs (i.e. using them whenever there is
any risk of noise exposure). Was it the therapy or was it the tincture of time that led me to a +50% improvement? I cannot answer that: I am a one-man study and statistics cannot be performed on one person alone. But I have shared my audiograms and shared the knowledge that I have. Some people have had a laugh at my expense saying my stem cell- and LLLT-treatments were a scam since I wasn't cured 100%, but if you compare my own results of +50%, that in fact - and in retrospect - is much more realistic if you compare it with the initial anecdotal results of volunteers of the AM-101 trial as well those who attempted Trobalt (i.e. the results are apparently
tangible, but
modest). So at least I have not been misleading the forum (I could easily have claimed a 100% success rate if I wanted to, in order to "not lose face", so to speak). From my own experience, a 50% improvement is the minimum necessary to regain basic functioning (when initially suffering from catastrophic tinnitus). On days where the improvement is around 70% better (vs. baseline) that is when I start to really feel human again, but I would say that a +80% improvement is necessary to "forget" that a person is suffering from tinnitus (when the initial comparison baseline is "severe tinnitus"). At least that is my own experience.
Still, I would not specifically recommend doing what I did. I only did what I did - in part - because clinical trials were not available to me as a Dane living in Germany. TRT and various hybrids of psychotherapies seem to remain the standard recommendation by the established medical community in the year 2015 for the treatment of subjective and non-treatable objective tinnitus.
attheedgeofscience
03/MAY/2015.

 Member
Member