
 Member
MemberDo you forget that initially they presented evidence that it reached all the way to the base of the cochlear by taking samples from people who were getting cochlear implants?They may not be talking about it but they are still measuring & tracking tinnitus in the currently enrolling Phase 2 trial. FX-322 may not work for everybody as it barely penetrates the first 15% of the cochlea. Some people's hearing loss may not be in that range. Also, do you know how many of those people you know received placebo?
If you hire a piano technician to come fix your piano but he only has the equipment and strings to work on 15% of it, do you expect him to be able to fix every piano he comes across?
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Frequency Therapeutics — Hearing Loss Regeneration
- Thread starter RB2014
- Start date
More options
Who Replied?I just don't understand these analogies.They may not be talking about it but they are still measuring & tracking tinnitus in the currently enrolling Phase 2 trial. FX-322 may not work for everybody as it barely penetrates the first 15% of the cochlea. Some people's hearing loss may not be in that range. Also, do you know how many of those people you know received placebo?
If you hire a piano technician to come fix your piano but he only has the equipment and strings to work on 15% of it, do you expect him to be able to fix every piano he comes across?
1. The hearing range people need the most is in the 125-8000 Hz range. The speech range is in the 125-5000 Hz range. FX-322 doesn't hit those frequencies. Frequency Therapeutics has had to temper expectations of the drug significantly (earlier presentations showed the drug hitting 4000 Hz).
2. We've seen some improvements with FX-322 in the earlier trials in the 8000 Hz range, but only in a handful of cases. The drug is unpredictable in this regard. And even then, it has only shown 10 dB improvement, which is within the margin of error. Lots of people with hearing loss have had 10 dB differences on audiograms on a certain frequency, including myself.
3. The drug hasn't shown improvements in ultra high frequencies, which they DID test in the latest trials. Which is weird if the theory is, is that the drug works fine, but remains in the base of the cochlea.
4. The drug focuses on speech recognition now. Great. Only 1 in 3 showed improvement in the trials. Those same trials suggest some people will lose their SR gains within two years. Getting a shot every two years for minimal benefit is not an alluring perspective. Intratympanic injections are not like COVID-19 shots. It's a lot more hassle. And if your hearing does decline in those two years, chances are you'd have to have your hearing aids adjusted as well, possibly multiple times. More hassle.
I don't dispute that FX-322 is a step in the right direction. But ultimately it will be something that comes before an actual treatment. Frequency Therapeutics' stock price seems to agree.
- Feb 14, 2020
- 1,630
- Tinnitus Since
- 1-2019
- Cause of Tinnitus
- 20+ Years of Live Music, Motorcycles, and Power Tools
These are good points. The heterogeneity of the patient population has been a problem for them since even the Phase 1/2 that caused a stir. And it's important to deeply understand that problem. The hearing loss each person experiences has a number of variables that cause it, even in just the groups with SNHL that this drug is intended to treat. What's compounds this problem is that the current clinical tests don't do a great job of differentiating subsets for recruiting/acceptance purposes. It shows very well in this slide:I just don't understand these analogies.
1. The hearing range people need the most is in the 125-8000 Hz range. The speech range is in the 125-5000 Hz range. FX-322 doesn't hit those frequencies. Frequency Therapeutics has had to temper expectations of the drug significantly (earlier presentations showed the drug hitting 4000 Hz).
2. We've seen some improvements with FX-322 in the earlier trials in the 8000 Hz range, but only in a handful of cases. The drug is unpredictable in this regard. And even then, it has only shown 10 dB improvement, which is within the margin of error. Lots of people with hearing loss have had 10 dB differences on audiograms on a certain frequency, including myself.
3. The drug hasn't shown improvements in ultra high frequencies, which they DID test in the latest trials. Which is weird if the theory is, is that the drug works fine, but remains in the base of the cochlea.
4. The drug focuses on speech recognition now. Great. Only 1 in 3 showed improvement in the trials. Those same trials suggest some people will lose their SR gains within two years. Getting a shot every two years for minimal benefit is not an alluring perspective. Intratympanic injections are not like COVID-19 shots. It's a lot more hassle. And if your hearing does decline in those two years, chances are you'd have to have your hearing aids adjusted as well, possibly multiple times. More hassle.
I don't dispute that FX-322 is a step in the right direction. But ultimately it will be something that comes before an actual treatment. Frequency Therapeutics' stock price seems to agree.
They didn't update for severe, but we basically know now that the drug doesn't have the desired effect if the PTA is worse than 85 dB. But just looking at this chart, they've tested FX-322 on a lot of different patient types. And, even the patient groups that show improvement, only 27% - 40% show any statistical improvement. At first glance, this looks like it "doesn't work well" or is underwhelming. But really, this goes back to the subset heterogeneity problem. This data shows that there just simply isn't a good way to predict based on clinical metrics (PTA, Audiogram, WS, WIN) how well the patient's hearing will improve with FX-322.
It appears with the 208 trial (Phase 2B) that they will be validating and accepting patients that fit in those 3 "most likely" subsets. They touched on this at R&D and in the Q&A. It's also literally circled in the slide. If they have enough information on what makes a responder from these likely subjects, they might be able to filter based on clinical metrics, or at least improve the odds of significant outcomes.
This information on the specific makeup of responders will inform the pivotal trial. Does this mean that the drug will only have an effect on potentially moderate -> severe SNHL cases PLUS whatever more distinct criteria they come up with for pivotal? It does not. It means the pivotal criteria defines the population the drug is known to have the most measurable effect with today's clinical metrics; and the patient population the FDA approves the drug for.
Their strategy was to cast a wide net to see if there were any uncovered opportunities. There were not. The stock price went south and some community support soured. Part of this, in my opinion, was poor communication on their part, and overcooked expectations by many on this forum and elsewhere.
Now it seems that they're working on improving the granularity of their recruiting criteria through pivotal. This should tilt the odds in their favor of picking quality responders reliably.
Chad Lawton
Member
- Mar 1, 2018
- 253
- Tinnitus Since
- 02/2018
- Cause of Tinnitus
- Possible Ototoxicity + Noise Exposure
No, I did not forget and yes, you are correct in that they showed FX-322 reaches the base of the cochlea... as it is right next to the round window membrane and where your high frequencies are located...Do you forget that initially they presented evidence that it reached all the way to the base of the cochlear by taking samples from people who were getting cochlear implants?
Sounds like you have your cochlear anatomy backwards and are under the impression that they made the claim FX-322 was reaching the apex of the cochlea but they never made such claim.
You might want to follow the company a little more closely going forward if you're going to be bad mouthing their drug...
Yep--which is because humans are very good at dealing with gaps in data--and with language usually leaning heavily on context. That's why we can read sentences full of typos and almost not even know the typos are there.Ah, keep telling yourself that. I have 45-50 WRS and I can't hear shit out of my left ear.
The press release made no claims about which region the drug and didn't hit.No, I did not forget and yes, you are correct in that they showed FX-322 reaches the base of the cochlea... as it is right next to the round window membrane and where your high frequencies are located...
Sounds like you have your cochlear anatomy backwards and are under the impression that they made the claim FX-322 was reaching the apex of the cochlea but they never made such claim.
You might want to follow the company a little more closely going forward if you're going to be bad mouthing their drug...
Frequency Therapeutics Shares Clinical Data From Exploratory Study Confirming Delivery of FX-322 to the Cochlea
I doubt it's even possible to determine the region of the cochlea the drug hits this way. I think they simply extracted perilymph and tested it for drug concentrations.
The thing that doesn't add up for me is that no improvements have been detected in the ultra high frequencies. Which is confusing if you believe the theory the drug works but is stuck in the base of the cochlea.
- Nov 29, 2014
- 211
- Tinnitus Since
- 10/2007
- Cause of Tinnitus
- Acoustic trauma - Repeated gun blasts
This is true and is why tinnitus is an anomaly and the vast majority of people will never experience tinnitus in their lifetime.Yep--which is because humans are very good at dealing with gaps in data--and with language usually leaning heavily on context. That's why we can read sentences full of typos and almost not even know the typos are there.
- Feb 14, 2020
- 1,630
- Tinnitus Since
- 1-2019
- Cause of Tinnitus
- 20+ Years of Live Music, Motorcycles, and Power Tools
This is what stemmed the discussion last year that perhaps IHC were preferentially regrown first or with only a single pass of injection. Speaking of the cells alone, The audiogram isn't a reliable measure of IHC condition, but is for OHC. Again, considering cell condition only, Word in quiet and word in noise tests are known to better measure IHC condition.The thing that doesn't add up for me is that no improvements have been detected in the ultra high frequencies. Which is confusing if you believe the theory the drug works but is stuck in the base of the cochlea.
So far, we've seen examples from Frequency Therapeutics where word in quiet (Phase 1/2, 1b) improve, but not really audiogram. And, word-in-noise in the Severe Phase 1b trial.
The evidence doesn't definitively point to IHC being regenerated and OHC not being regenerated. However it does show there may be a tendency for IHC preference in a specific subset of SNHL patients.
Chad Lawton
Member
- Mar 1, 2018
- 253
- Tinnitus Since
- 02/2018
- Cause of Tinnitus
- Possible Ototoxicity + Noise Exposure
Keep in mind how few hair cells & "sq footage" for hair cells are dedicated to the high frequency regions in the cochlea. Look at most cochlear diagrams and there are as many hair cells dedicated to between 8 kHz to 20 kHz range as there are dedicated to the 6 kHz to 8 kHz range. Pair that with their preclinical imaging of the mouse cochlea where the highest frequency regions don't appear to respond as well to FX-322 as the lower ones.The thing that doesn't add up for me is that no improvements have been detected in the ultra high frequencies. Which is confusing if you believe the theory the drug works but is stuck in the base of the cochlea.
Attachments
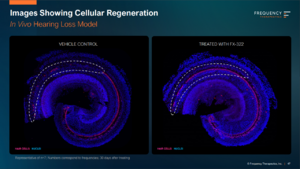
Why doesn't it work at the base of the cochlea?Keep in mind how few hair cells & "sq footage" for hair cells are dedicated to the high frequency regions in the cochlea. Look at most cochlear diagrams and there are as many hair cells dedicated to between 8 kHz to 20 kHz range as there are dedicated to the 6 kHz to 8 kHz range. Pair that with their preclinical imaging of the mouse cochlea where the highest frequency regions don't appear to respond as well to FX-322 as the lower ones.
Sorry I used the wrong word. But you obviously aren't following them closely enough because the drug doesn't work. It may work in a lab setting but it doesn't work on humans.No, I did not forget and yes, you are correct in that they showed FX-322 reaches the base of the cochlea... as it is right next to the round window membrane and where your high frequencies are located...
Sounds like you have your cochlear anatomy backwards and are under the impression that they made the claim FX-322 was reaching the apex of the cochlea but they never made such claim.
You might want to follow the company a little more closely going forward if you're going to be bad mouthing their drug...
Chad Lawton
Member
- Mar 1, 2018
- 253
- Tinnitus Since
- 02/2018
- Cause of Tinnitus
- Possible Ototoxicity + Noise Exposure
That is a question we don't have an answer to. Maybe the small molecule combination is too potent at the base. Maybe hair cells in the highest frequencies are more easily prone to noise damage while healing based on their proximity to the eardrum. We don't know. The science will get clearer over time.Why doesn't it work at the base of the cochlea?
Chad Lawton
Member
- Mar 1, 2018
- 253
- Tinnitus Since
- 02/2018
- Cause of Tinnitus
- Possible Ototoxicity + Noise Exposure
I'm not going to waste anymore time engaging you then since you refuse to follow the science and are making false claims about FX-322. All the data FREQ has provided suggests FX-322 works but you refuse to accept any of it. Just because it doesn't touch your audiograms or you specifically will be unlikely to benefit from it; it doesn't mean millions of other people won't.Sorry I used the wrong word. But you obviously aren't following them closely enough because the drug doesn't work. It may work in a lab setting but it doesn't work on humans.
Then why did I get contacted for the trial?Just because it doesn't touch your audiograms or you specifically will be unlikely to benefit from it; it doesn't mean millions of other people won't.
I am exactly who it is intended to treat.
Moderate sudden hearing loss.
Keith Handy
Member
- Jan 5, 2021
- 302
- Tinnitus Since
- 11/2020
- Cause of Tinnitus
- Stress + sleep deprivation + noise
True, but there is no context given for the words in these tests.Yep--which is because humans are very good at dealing with gaps in data--and with language usually leaning heavily on context. That's why we can read sentences full of typos and almost not even know the typos are there.
Possibly, but that would only make sense if supporting cells responsible for regrowth of IHC respond better to the drug somehow. Why would that be the case? It wasn't the case in pre-clinical work. Supporting cells are supporting cells. Furthermore, I haven't heard Frequency Therapeutics give that explanation. The way to see if this theory holds up is to examine cochleas of people who have gotten the drug.This is what stemmed the discussion last year that perhaps IHC were preferentially regrown first or with only a single pass of injection. Speaking of the cells alone, The audiogram isn't a reliable measure of IHC condition, but is for OHC. Again, considering cell condition only, Word in quiet and word in noise tests are known to better measure IHC condition.
So far, we've seen examples from Frequency Therapeutics where word in quiet (Phase 1/2, 1b) improve, but not really audiogram. And, word-in-noise in the Severe Phase 1b trial.
The evidence doesn't definitively point to IHC being regenerated and OHC not being regenerated. However it does show there may be a tendency for IHC preference in a specific subset of SNHL patients.
- Feb 14, 2020
- 1,630
- Tinnitus Since
- 1-2019
- Cause of Tinnitus
- 20+ Years of Live Music, Motorcycles, and Power Tools
Like I said, it was a discussion here between some of the members that have done quite a bit of due diligence on prior work and the human cochlea. Lots of shared research on how the cochlea develops, the role of the IHC/OHC, and how Frequency Therapeutics describes the function of FX-322 in patents, which can be very revealing.Possibly, but that would only make sense if supporting cells responsible for regrowth of IHC respond better to the drug somehow. Why would that be the case? It wasn't the case in pre-clinical work. Supporting cells are supporting cells. Furthermore, I haven't heard Frequency Therapeutics give that explanation. The way to see if this theory holds up is to examine cochleas of people who have gotten the drug.
Frequency Therapeutics has said numerous times that they have observed IHC and OHC regenerated by human cochlea tissue in vitro.
Perhaps supporting cells aren't all created equal as you say. In Frequency Therapeutics' patents, they cite LGR5+ supporting cells as the target for the drug, acknowledging that supporting cells that are NOT LGR5+ exist in some embodiment within the cochlea, and are of no use to the mechanisms in the drug.
They're also at a limit to what they can publicly disclose without bonafide validation. So, if they can't show for-sure that a living person received FX-322 and their cochleas regenerated either IHC or OHC or both, they really can only rely on the clinical measures available in the trials; and those trials aren't specific enough to rule out either or rule in either.
It's possible the living cochlea tissue has another mechanism at play that limits activation of progenitors to some extent. If you recall, the concept of progenitor cell activation is to trigger a program in those LGR5+ support cells to perform mitosis that they only did once in all of us in utero, never to be activated again. These are uncharted waters.
Unfortunately, ambiguity seems to be the realm these companies rely upon to draw their preferred conclusions. I just don't buy the idea that there are insufficient clinical measures available to judge a treatment's efficacy. It may be a fuzzier domain than other areas of medicine, but not as fuzzy as these companies make it seem.they really can only rely on the clinical measures available in the trials; and those trials aren't specific enough to rule out either or rule in either.
- Feb 14, 2020
- 1,630
- Tinnitus Since
- 1-2019
- Cause of Tinnitus
- 20+ Years of Live Music, Motorcycles, and Power Tools
If there are better methods that are validated and approved by the FDA, why aren't they using them? Why aren't they cited in any publicly available research?Unfortunately, ambiguity seems to be the realm these companies rely upon to draw their preferred conclusions. I just don't buy the idea that there are insufficient clinical measures available to judge a treatment's efficacy. It may be a fuzzier domain than other areas of medicine, but not as fuzzy as these companies make it seem.
Koz
Member
- Dec 15, 2013
- 153
- Tinnitus Since
- 2009
- Cause of Tinnitus
- Unilateral sensorineural hearing loss
Mmmm, another day closer to celebrating recognising words rather than the vast majority of sounds in the wide range/spectrum of sound frequencies
Don't get me wrong, I don't take joy in being some kind of party pooper or being negative, in fact I am rooting for Frequency Therapeutics (and everyone else in this field) but as someone with a full flat severe hearing loss in one ear, for me WRS as a measure of drug effectiveness is laughable. I understand significant Audiogram improvement might come later down the line with FX-322 or FX-325 but until clinical results of that are published then it's all hope on little things and excuses, a recurrent theme in this thread.
They sure have talked the talk but are still a long way to go, more than originally expected with some bits of hope to keep us going.
I mean I'd be hyped if I got excited for stuff at a snail's pace or if I was one of em "I have no visible loss on the audiogram but still have tinnitus/funny hearing" people - which I am not, I am almost full blown deaf in one ear, so this is merely the view from the other side.
Sure Rome wasn't built in a day but the schematics of the Colosseum are not the actual Colosseum. Until then:

Don't get me wrong, I don't take joy in being some kind of party pooper or being negative, in fact I am rooting for Frequency Therapeutics (and everyone else in this field) but as someone with a full flat severe hearing loss in one ear, for me WRS as a measure of drug effectiveness is laughable. I understand significant Audiogram improvement might come later down the line with FX-322 or FX-325 but until clinical results of that are published then it's all hope on little things and excuses, a recurrent theme in this thread.
They sure have talked the talk but are still a long way to go, more than originally expected with some bits of hope to keep us going.
I mean I'd be hyped if I got excited for stuff at a snail's pace or if I was one of em "I have no visible loss on the audiogram but still have tinnitus/funny hearing" people - which I am not, I am almost full blown deaf in one ear, so this is merely the view from the other side.
Sure Rome wasn't built in a day but the schematics of the Colosseum are not the actual Colosseum. Until then:
Why don't you get a cochlear implant?Mmmm, another day closer to celebrating recognising words rather than the vast majority of sounds in the wide range/spectrum of sound frequencies
Don't get me wrong, I don't take joy in being some kind of party pooper or being negative, in fact I am rooting for Frequency Therapeutics (and everyone else in this field) but as someone with a full flat severe hearing loss in one ear, for me WRS as a measure of drug effectiveness is laughable. I understand significant Audiogram improvement might come later down the line with FX-322 or FX-325 but until clinical results of that are published then it's all hope on little things and excuses, a recurrent theme in this thread.
They sure have talked the talk but are still a long way to go, more than originally expected with some bits of hope to keep us going.
I mean I'd be hyped if I got excited for stuff at a snail's pace or if I was one of em "I have no visible loss on the audiogram but still have tinnitus/funny hearing" people - which I am not, I am almost full blown deaf in one ear, so this is merely the view from the other side.
Sure Rome wasn't built in a day but the schematics of the Colosseum are not the actual Colosseum. Until then:
View attachment 48604
- Feb 14, 2020
- 1,630
- Tinnitus Since
- 1-2019
- Cause of Tinnitus
- 20+ Years of Live Music, Motorcycles, and Power Tools
Yes because hearing 9 specific beeps an octave apart == hearing a wide range/spectrum of sounds. I didn't know we communicate in 90's modem sounds to each other.the vast majority of sounds in the wide range/spectrum of sound frequencies
I'm still wrestling to understand all these false expectations airings on this thread that blister up from time to time. There's not a single example of a treatment for any other degenerative disease that is developed faster than a snails pace. Why would hearing loss be any different? Considering the scope of progress made to understand and treat human hearing over the past 100 years, where the first 80 or so led to the production of the cochlear implant, I'd say the recent developments in the last 5 years are moving at a really impressive clip. All one has to do is look at the past 2 years and observe the number of potential drugs to treat different hearing loss etiologies in the pipeline. These aren't academic research projects, either, these are commercially backed projects built on top of published science. 10 years ago, there was maybe 1.
So yeah, I guess if you're part the crowd that demands instant gratification, I could see how you might be disappointed.
No human in hundreds of thousands of years of existence on Earth have ever been able to renew their hearing biology. Yet, in the most recent 5 years of human existence, there have been multiple examples of treatments that show promise to overturn that biological law. In my opinion, that's science happening at warp speed.
Geatly
Member
- Jan 17, 2022
- 70
- Tinnitus Since
- 12/2021
- Cause of Tinnitus
- Noise induced, by jackhammering into concrete on constructio
Yeah, they didn't need to renew their hearing biology, because in the first place there was nothing that could damage it, no live concerts, no power tools, no jackhammers etc etc.Yes because hearing 9 specific beeps an octave apart == hearing a wide range/spectrum of sounds. I didn't know we communicate in 90's modem sounds to each other.
I'm still wrestling to understand all these false expectations airings on this thread that blister up from time to time. There's not a single example of a treatment for any other degenerative disease that is developed faster than a snails pace. Why would hearing loss be any different? Considering the scope of progress made to understand and treat human hearing over the past 100 years, where the first 80 or so led to the production of the cochlear implant, I'd say the recent developments in the last 5 years are moving at a really impressive clip. All one has to do is look at the past 2 years and observe the number of potential drugs to treat different hearing loss etiologies in the pipeline. These aren't academic research projects, either, these are commercially backed projects built on top of published science. 10 years ago, there was maybe 1.
So yeah, I guess if you're part the crowd that demands instant gratification, I could see how you might be disappointed.
No human in hundreds of thousands of years of existence on Earth have ever been able to renew their hearing biology. Yet, in the most recent 5 years of human existence, there have been multiple examples of treatments that show promise to overturn that biological law. In my opinion, that's science happening at warp speed.
You're confusing criticizing a drug for its efficacy and instant gratification. Frequency Therapeutics themselves didn't talk about word recognition until after the first trials didn't show audiogram improvements. We as patients have no holy obligation to morally support any particular drug. I wish every hearing scientist the best and I'm glad they're here, but at the end of the day all that matters are the results.Yes because hearing 9 specific beeps an octave apart == hearing a wide range/spectrum of sounds. I didn't know we communicate in 90's modem sounds to each other.
I'm still wrestling to understand all these false expectations airings on this thread that blister up from time to time. There's not a single example of a treatment for any other degenerative disease that is developed faster than a snails pace. Why would hearing loss be any different? Considering the scope of progress made to understand and treat human hearing over the past 100 years, where the first 80 or so led to the production of the cochlear implant, I'd say the recent developments in the last 5 years are moving at a really impressive clip. All one has to do is look at the past 2 years and observe the number of potential drugs to treat different hearing loss etiologies in the pipeline. These aren't academic research projects, either, these are commercially backed projects built on top of published science. 10 years ago, there was maybe 1.
So yeah, I guess if you're part the crowd that demands instant gratification, I could see how you might be disappointed.
No human in hundreds of thousands of years of existence on Earth have ever been able to renew their hearing biology. Yet, in the most recent 5 years of human existence, there have been multiple examples of treatments that show promise to overturn that biological law. In my opinion, that's science happening at warp speed.
- Feb 14, 2020
- 1,630
- Tinnitus Since
- 1-2019
- Cause of Tinnitus
- 20+ Years of Live Music, Motorcycles, and Power Tools
Ancient Egyptians, Greeks, Romans made record of hearing loss and tinnitus.Yeah, they didn't need to renew their hearing biology, because in the first place there was nothing that could damage it, no live concerts, no power tools, no jackhammers etc etc.
Geatly
Member
- Jan 17, 2022
- 70
- Tinnitus Since
- 12/2021
- Cause of Tinnitus
- Noise induced, by jackhammering into concrete on constructio
Actually that is not that far away in time, when you realize it's just 2000-3000 years back in timeline, which is just a drop when we know that humans have been more than 300 000 years on this planet. Of course they could experience hearing loss and tinnitus because by that time there were already tools and works that were noisy, for example when pyramids were being built or anything like that, it had to be done by ordinary slaves with hard work and it probably was noisy. Same goes for wars. In battle or whatever there was exceeding noise exposure etc. Something our auditory system wasn't used to before.Ancient Egyptians, Greeks, Romans made record of hearing loss and tinnitus.
- Feb 14, 2020
- 1,630
- Tinnitus Since
- 1-2019
- Cause of Tinnitus
- 20+ Years of Live Music, Motorcycles, and Power Tools
Around 3000BC, Ancient Egyptians may have been using tools. So, let's say the scope of tool use that could have caused hearing loss is 5000 years. My argument that the last 5 years of progress is happening at warp speed compared to the 5000 years of known tool use (that may have caused hearing loss) is still valid.Actually that is not that far away in time, when you realize it's just 2000-3000 years back in timeline, which is just a drop when we know that humans have been more than 300 000 years on this planet. Of course they could experience hearing loss and tinnitus because by that time there were already tools and works that were noisy, for example when pyramids were being built or anything like that, it had to be done by ordinary slaves with hard work and it probably was noisy. Same goes for wars. In battle or whatever there was exceeding noise exposure etc. Something our auditory system wasn't used to before.
DimLeb
Member
- Jun 20, 2021
- 368
- Tinnitus Since
- 03/2021
- Cause of Tinnitus
- Idiopathic Cochleopathy or Maybe Loud Music
There always were presbycusis, idiopathic causes, inner ear diseases, physical injuries and maybe some loud noise events (working in mines, war etc)... Just saying, the need was always there unfortunately, but nothing could be done.Yeah, they didn't need to renew their hearing biology, because in the first place there was nothing that could damage it, no live concerts, no power tools, no jackhammers etc etc.