
 Member
Member- Jan 5, 2020
- 90
- Tinnitus Since
- 2011, Spike 2019, Spike 2020
- Cause of Tinnitus
- 1e Loud Music, 2e earwax irrigation, 3e padel tennis
She replied:
"We hope not"
I believe it will impact some of the details of the trial, but not the grand picture. They will still eventually be able to measure MML / loudness which can serve as the basis of a comparison, and TFI / THI scores will certainly also be a good indicator especially if the reduction is large.Hi. The trial is impacted by COVID19, but it is not clear if that will delay the timeline. It may limit how large the population is in the trial, and what aspects of the data they can use, or at least apply to the whole population of participants. Right now, they cannot have participants come into the lab, which is the largest issue. Folks that are still on devices are asked to still use them. They are still sending TFI / THI surveys weekly to those on devices and in the washout period. They cannot measure pitch, MML, frequency, loudness etc as they do that in-lab in a controlled soundproof booth. I do think they are figuring out how they can use what they have in various forms. It's anyone's guess as to when they can have people back in the lab.
I would not expect any report before late Q3, 2020.
Hi. The trial is impacted by COVID19, but it is not clear if that will delay the timeline. It may limit how large the population is in the trial, and what aspects of the data they can use, or at least apply to the whole population of participants. Right now, they cannot have participants come into the lab, which is the largest issue. Folks that are still on devices are asked to still use them. They are still sending TFI / THI surveys weekly to those on devices and in the washout period. They cannot measure pitch, MML, frequency, loudness etc as they do that in-lab in a controlled soundproof booth. I do think they are figuring out how they can use what they have in various forms. It's anyone's guess as to when they can have people back in the lab.
I would not expect any report before late Q3, 2020.
Thanks for the info. Since you seem well informed on the subject, do you know or could you guess what part of the trial population until this point has been affected because of the lockdown?
I imagine you have a NDA, but I have to ask whether you have any hope to share with us. I think we could all use a good shot of hope right now. Did it help you?I know they were just about done recruiting, which means they were close to their target population at least starting if not fully completed. This is good news because even if a portion dropped off, they likely have a lot of data. Specific numbers, I'm not sure, but I do think they'll have enough to study and publish. It won't be as large as expected but it will be enough. And they may be able to draw broader conclusions by augmenting the core data with some of the less compete subjects data too.
I am in the study and sharing what's I have learned about the trajectory of their work through their direct communications about COVID.
She wouldn't want to be another Michael Kilgard.I believe that Susan Shore is too arrogant to allow her name to be sullied by an underperforming device. She would rather release nothing than risk being snubbed at faculty cocktail parties.
Hey there - I would absolutely hate to give you my one, isolated, anecdotal (because no one has the data available) perception of this study and the device's effect on my tinnitus. I'd also hate to say anything to compromise the study.I imagine you have a NDA, but I have to ask whether you have any hope to share with us. I think we could all use a good shot of hope right now. Did it help you?
So the clinical trial has already started?I know they were just about done recruiting, which means they were close to their target population at least starting if not fully completed. This is good news because even if a portion dropped off, they likely have a lot of data. Specific numbers, I'm not sure, but I do think they'll have enough to study and publish. It won't be as large as expected but it will be enough. And they may be able to draw broader conclusions by augmenting the core data with some of the less compete subjects data too.
I am in the study and sharing what's I have learned about the trajectory of their work through their direct communications about COVID.
You mean you couldn't use pillows sleeping on your back? Mine was the same. I went to a chiro that uses a "Y strap" (go to YouTube and search) and it helps my neck with range of motion, but not my tinnitus.I haven't yet but looking into it, since no doubt my neck is always bad. I can't even use pillows because it hurts my neck at night. But that's encouraging that getting physical therapy for your neck relieved your tinnitus a lot. Gives me some hope to heal.
You mean you couldn't use pillows sleeping on your back? Mine was the same. I went to a chiro that uses a "Y strap" (go to YouTube and search) and it helps my neck with range of motion, but not my tinnitus.
You might be in the sham treatment arm so even if would be negatives it would not matter.Hey there - I would absolutely hate to give you my one, isolated, anecdotal (because no one has the data available) perception of this study and the device's effect on my tinnitus. I'd also hate to say anything to compromise the study.
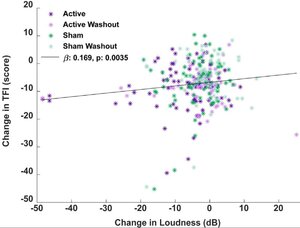
If you remove the outliers I don't think this plot looks much better than Lenire, TBH. Not really encouraging the way the sham results are almost identical with actual active treatment--strongly implying placebo.You might be in the sham treatment arm so even if would be negatives it would not matter.
I did small computation based on https://stm.sciencemag.org/content/scitransmed/10/422/eaal3175.full.pdf
They said "Tinnitus reduction reached an average of 12.2 dB in the fourth week of active treatment. Of the 20 participants tested, 2 reported complete elimination of their tinnitus toward the end of the active treatment period."
I interpreted from the figure below that those "two" had reduction of 49dB and 47dB. Given that we know the end results of those "two" super responders how much is the average reduction of the rest of the 18 patients. Turns out it is 8.22 dB which is still more than any of the sham treatment weeks (figure 6 a in the paper)
I have to disagree. Even after removal of "the super two" the treatment shows benefits. See figure.If you remove the outliers I don't think this plot looks much better than Lenire, TBH. Not really encouraging the way the sham results are almost identical with actual active treatment--strongly implying placebo.
Which device is coming out first to the market, UMinn or UMich? Or which device is going to complete the clinical trials and publish study results first?I'd like to see similar result data for Minnesota. @kelpiemsp's testimonial made me think that was the most promising of all.
Also how do they figure out the decibel reduction in these cases? What is the difference between active and active washout?I have to disagree. Even after removal of "the super two" the treatment shows benefits. See figure.
Also Lenire paper (if you are referring to this one [1]) had no sham group. Simulation took 10 weeks in Lenire paper vs. 4 weeks.
[1] https://www.neuromoddevices.com/con...dvancement/phase-i-safety-and-feasibility.pdf)
Overall Shore's results appears much much stronger. Will it cure us all? Probably not but if 10% are totally cured and others get some benefits then it is already the best result tinnitus world has seen outside of maybe Benzos or Trobalt that have very serious side effects.
View attachment 38219
Washout = No Treatment. Decibel reduction I don't knowAlso how do they figure out the decibel reduction in these cases? What is the difference between active and active washout?
I asked Susan Shore via e-mail if her treatment is for somatic tinnitus only, and this is what I received: 'Regarding somatic tinnitus, that is the kind we have been researching, but it could be that our treatment is also effective for those who cannot modulate'.
It seems lack of somatic elements will not exclude one from being treated.
This is what she replied to me a month ago:Anyone hear anything new on the trial results or commercialization of Shore's device?
")