
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Otonomy OTO-413 — Treatment of Hidden Hearing Loss
- Thread starter Michael Larsen
- Start date
More options
Who Replied?Geatly
Member
- Jan 17, 2022
- 70
- Tinnitus Since
- 12/2021
- Cause of Tinnitus
- Noise induced, by jackhammering into concrete on constructio
That is because FX-345 is actually second generation. Well that would be amazing. I think it will, even more than just 20 dB.What if FX-345 shows improvements of at least 20 dB in audiograms?
 Member
Member- Feb 14, 2020
- 1,630
- Tinnitus Since
- 1-2019
- Cause of Tinnitus
- 20+ Years of Live Music, Motorcycles, and Power Tools
They noted at the beginning of the webcast that the patients recruited in Phase 2A had hearing that was worse on-average than those in the Phase 1/2. It seems to me considering how heterogeneous hearing loss is, that a worse group probably also has greater variations between each individuals in extent and type of damage. So that may explain the lower % of responders.I was wondering why investors don't seem to care about the results. So I compared them with the Phase 1/2 results and this does curb my enthusiasm a bit.
40% vs 67% OTO-413 subjects demonstrated a clinically-meaningful improvement on at least one of the three SIN tests at both Days 57 and 85.
15% vs 33% OTO-413 subjects demonstrated a clinically-meaningful improvement by two or more different SIN tests at both Days 57 and 85.
Still clearly better than the placebo group though.
Good news is in a few months, we'll learn about how the higher dosages may have a greater effect to a similar group.
They also have the option to p-hack their drug population like Frequency Therapeutics is doing with FX-322, by just recruiting baselines that show the highest likelihood of responding to drug. Which they will know before the"full" Phase 2.
One of the inclusion criteria was:I have looked at the presentation, and I understand that OTO-413 will only be suitable for moderate / severe hearing loss but not for profound hearing loss (over 90 dB): is that correct? So whoever has profound hearing loss will not find any benefit from either OTO-413 or FX-345?
- Subject has audiometrically-defined normal hearing or up to moderately severe hearing impairment.
Skydog07
Member
It's the most prominent one, and it's the only hearing drug to have positive results in 2 trials so far - however, it's not the only drug currently being tested for hidden hearing loss. Pipeline Therapeutics' PIPE-505 also aims to do this, but their Phase 1/2a study ended mid-last year and they have yet to release the results. That sort of signals to me that the results weren't that impressive.Is OTO-413 the main treatment for hidden hearing loss patients to look forward to?
The current phase should be ending this month, right?
We should hear something between August and the end of this year regarding the higher dosage trials (my guess is in September). Hopefully they'll yield improved results.I hope further news comes out soon.
Geatly
Member
- Jan 17, 2022
- 70
- Tinnitus Since
- 12/2021
- Cause of Tinnitus
- Noise induced, by jackhammering into concrete on constructio
Patient Global Impression of Change. It's written down on the paper.What is PGIC on the graph?
We don't know if there will be a hearing loss treatment now or even 10-15 years later. Best thing to do is to wait for the results of the ongoing clinical trials, especially FX-345 and from there on, we decide how soon we will have a cure.Being realistic, not pessimistic, I would think all the hearing regeneration drugs are 10-15 years away. I would like to hear differing opinions obviously.
Also, I don't understand why you are pessimistic. I don't think you are being realistic. FX-322 has shown to improve hearing in WR tests. Same applies to OTO-413. There is also OTO-6XX on the horizon, which has not even been tested yet...
My advice to you is to wait for FX-345 results before killing all of us.
When we have those results? This year?My advice to you is to wait for FX-345 results before killing all of us.
In the first half of next year (by June 2023 the latest).When we have those results? This year?
OTO-413 - the thread you're in - is probably only a few years away. Its shown in 2 trials now to improve hearing in 40-60% of patients. That may not seem amazing initially, but consider these additional points:Being realistic, not pessimistic, I would think all the hearing regeneration drugs are 10-15 years away. I would like to hear differing opinions obviously.
- They're currently running trials on 2.5x and 5x the dosage of the Phase 2a trial.
- They're considering giving a second dose in the next trial (it'll probably depend on how well the 5x dosage does).
- They're considering dosing both ears in future trials (since people hear with both ears and it may be easier to show the effect).
With these enhancements we may see a significantly larger percentage of patients showing a benefit.
However, if you're looking for a blockbuster drug that will fix completely hearing, yeah, I think we're a long ways away - and that may not even be possible. It's looking more and more likely that we'll need to take different drugs to fix different parts of the cochlea (synapses, inner hair cells, outer hair cells, etc etc).
Even that is pretty amazing considering how heterogeneous hearing loss is. IIRC Otonomy didn't set any specific criteria for how participants got hearing loss or how long they had it for. I'm all for cautious optimism and not putting your eggs in one basket, but I think there's reason to be hopeful here.OTO-413 - the thread you're in - is probably only a few years away. Its shown in 2 trials now to improve hearing in 40-60% of patients. That may not seem amazing initially
I couldn't agree more. I try not to be too optimistic and get my hopes down, but OTO-413 compared to placebo was really good. Placebo was like 0 in most of the results. And like you said, more trials to come. I think OTO-413 will definitely hit the market, could be by 2025-2026. Unless things go horribly wrong.OTO-413 - the thread you're in - is probably only a few years away. Its shown in 2 trials now to improve hearing in 40-60% of patients. That may not seem amazing initially, but consider these additional points:
- They're currently running trials on 2.5x and 5x the dosage of the Phase 2a trial.
- They're considering giving a second dose in the next trial (it'll probably depend on how well the 5x dosage does).
- They're considering dosing both ears in future trials (since people hear with both ears and it may be easier to show the effect).
With these enhancements we may see a significantly larger percentage of patients showing a benefit.
However, if you're looking for a blockbuster drug that will fix completely hearing, yeah, I think we're a long ways away - and that may not even be possible. It's looking more and more likely that we'll need to take different drugs to fix different parts of the cochlea (synapses, inner hair cells, outer hair cells, etc etc).
I don't have all my marbles on Frequency Therapeutics, but I do think their drug has potential. Just bad trial design.
You're right, expecting the first gen of drugs to cure profound deafness is not realistic at all. But treating hair cells and synapses, even getting 10 dB of hearing back is amazing progress.
- Dec 18, 2015
- 619
- 46
- Tinnitus Since
- 03/2015
- Cause of Tinnitus
- Noise induced, loud rock concert
What worries me about OTO-413 is that they refuse to consider tinnitus even as a secondary measure. What's more, they even have tinnitus listed as exclusion criteria.I couldn't agree more. I try not to be too optimistic and get my hopes down, but OTO-413 compared to placebo was really good. Placebo was like 0 in most of the results. And like you said, more trials to come. I think OTO-413 will definitely hit the market, could be by 2025-2026. Unless things go horribly wrong.
I don't have all my marbles on Frequency Therapeutics, but I do think their drug has potential. Just bad trial design.
You're right, expecting the first gen of drugs to cure profound deafness is not realistic at all. But treating hair cells and synapses, even getting 10 dB of hearing back is amazing progress.
They could have at least allowed tinnitus patients in a trial to leave space for any anecdotal evidence, like Frequency Therapeutics did with FX-322.
Would repairing hair cells take away the tinnitus in the brain? The maladaptive pathways in several areas of the brain caused by hearing damage?
This is the big question as well!
This is likely a direct nod to the FX-322 trials, and has been discussed at length in the OTO-6XX thread (@patorjk did a great job of hunting for and documenting every little scrap of information about it). The short version is that it seems Otonomy wants to try a different approach with OTO-6XX, focusing more on repair than regeneration. But they haven't put out anything concrete yet, so we don't know.
In any case, it might be better to continue that discussion in the OTO-6XX thread.
Perhaps, or perhaps Frequency Therapeutics has better tech. Time will tell.
Oh yeah, makes sense. Well remember, they got OTO-313 for tinnitus so I'm guessing they don't want any confusion or correlation between the two. My noxacusis is way more of an issue so that's why I'm excited for OTO-413. I wouldn't be too concerned on them not having anything to do with tinnitus for that drug because it will probably help if it's repairing synapses. There's probably other reasons I'm not thinking of but if those drugs fail trials, even if they work, the company goes under.What worries me about OTO-413 is that they refuse to consider tinnitus even as a secondary measure. What's more, they even have tinnitus listed as exclusion criteria.
They could have at least allowed tinnitus patients in a trial to leave space for any anecdotal evidence, like Frequency Therapeutics did with FX-322.
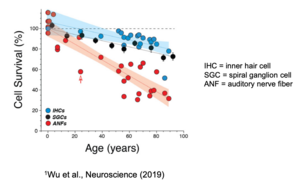
Synapses being the source of tinnitus doesn't make any sense. Check out these charts (they're from Otonomy and Decibel Therapeutics' corporate slide decks):What worries me about OTO-413 is that they refuse to consider tinnitus even as a secondary measure. What's more, they even have tinnitus listed as exclusion criteria.
They could have at least allowed tinnitus patients in a trial to leave space for any anecdotal evidence, like Frequency Therapeutics did with FX-322.
They show inner hair cell (IHC) survival, outer hair cell (OHC) survival, and synapse survival as we age. Both OHCs and synapses die off significantly as we get older. If tinnitus was causally linked to synapse death then tinnitus would be associated with getting old - yet not all old people have tinnitus. Instead it seems to be linked to cochlear injury.
Synapses have been linked to hearing-in-noise, which is why they're focusing on that. In fact, I think their studies might be the first to confirm synapses do in fact help with hearing-in-noise - but I'm not 100% on that.
If they were to measure tinnitus too, it might cause a bunch of people to join simply for that reason, leading to a situation similar to what happened with FX-322 in its Phase 2a trial (Frequency Therapeutics believes people faked their word scores to get into the study and messed up the placebo group).
As a final aside, people with non-bothersome tinnitus have been allowed into the previous studies. According to the last Tinnitus Talk Podcast interview, there were no anecdotes of OTO-413 helping with tinnitus.
Attachments

How is it possible to only help hearing loss but not tinnitus?Synapses being the source of tinnitus doesn't make any sense. Check out these charts (they're from Otonomy and Decibel Therapeutics' corporate slide decks):
View attachment 50589View attachment 50590
They show inner hair cell (IHC) survival, outer hair cell (OHC) survival, and synapse survival as we age. Both OHCs and synapses die off significantly as we get older. If tinnitus was causally linked to synapse death then tinnitus would be associated with getting old - yet not all old people have tinnitus. Instead it seems to be linked to cochlear injury.
Synapses have been linked to hearing-in-noise, which is why they're focusing on that. In fact, I think their studies might be the first to confirm synapses do in fact help with hearing-in-noise - but I'm not 100% on that.
If they were to measure tinnitus too, it might cause a bunch of people to join simply for that reason, leading to a situation similar to what happened with FX-322 in its Phase 2a trial (Frequency Therapeutics believes people faked their word scores to get into the study and messed up the placebo group).
As a final aside, people with non-bothersome tinnitus have been allowed into the previous studies. According to the last Tinnitus Talk Podcast interview, there were no anecdotes of OTO-413 helping with tinnitus.
Cochlear injury (which results in tinnitus) causes hearing loss (or hidden hearing loss), or is this not the case? Do I understand things wrong?
Why not? If synaptopathy leads to fewer/aberrant signals being sent to the brain, this could result in tinnitus.Synapses being the source of tinnitus doesn't make any sense.
One could make the same argument about cochlear injury though: not all people who have hearing loss have tinnitus. Also, tinnitus is associated with getting old; older people are more likely to have tinnitus, and their tinnitus is louder.Both OHCs and synapses die off significantly as we get older. If tinnitus was causally linked to synapse death then tinnitus would be associated with getting old - yet not all old people have tinnitus. Instead it seems to be linked to cochlear injury.
You could argue that people with, say, a noise injury are much more likely to develop tinnitus than people who simply get older. This makes intuitive sense to me but I have not seen any data that proves it.
Cochlear injury is one piece of the puzzle. It leads to fewer (or aberrant) signals being sent to the brain, who now has to make sense of these signals. Some are able to reorganize in a way that doesn't lead to tinnitus (as Dirk De Ridder says, "if the brain doesn't care that you have hearing loss (...) then it won't create the sounds"). Some are not, and that maladaptation leads to chronic tinnitus. There's more information about the role of the brain in the excellent models of tinnitus document that TinnitusTalk put out.How is it possible to only help hearing loss but not tinnitus?
Cochlear injury (which results in tinnitus) causes hearing loss (or hidden hearing loss), or is this not the case? Do I understand things wrong?
I'm not saying you're doing this, but it is common to see people here "picking sides", i.e. arguing very emphatically that tinnitus is either "in the ear" or "in the brain". This baffles me a little since all the research seems to show that it is in both. In the case of noise exposure, it starts with the ear, but the brain is involved. The hope is that fixing the ear also leads to fixing the brain. Likewise, fixing the brain could also help, even if the ear remains damaged. All that remains to be seen though.