
Came across this article...
http://www.eurekalert.org/pub_releases/2015-08/uops-pti082715.php
http://www.eurekalert.org/pub_releases/2015-08/uops-pti082715.php
PITTSBURGH, Aug. 27, 2015 - Researchers have identified in an animal model the molecular mechanisms behind resilience to noise-induced tinnitus and a possible drug therapy that could reduce susceptibility to this chronic and sometimes debilitating condition. The findings by a team from the University of Pittsburgh School of Medicine were published online in the journal eLife.
Tinnitus is typically induced by exposure to loud noise and causes whistling, clicking, roaring and other phantom sounds. It is estimated that 5 to 15 percent of Americans suffer from tinnitus, said Thanos Tzounopoulos, Ph.D., associate professor and member of the auditory research group in the Department of Otolaryngology, Pitt School of Medicine, where he also holds the auditory physiology endowed chair.
The study results build on previous research in mouse models demonstrating that tinnitus is associated with hyperactivity of dorsal cochlear nucleus (DCN) cells, which fire impulses even when there is no actual sound to perceive. The team's work has shown that this hyperactivity is caused by a reduction in tiny channels, called KCNQ channels, through which potassium ions travel in and out of the cell. Based on this finding, KCNQ channel activators have emerged as clinical candidates for preventing the development of tinnitus.
"However, a significant percentage of people are exposed to loud sounds and never develop tinnitus, and there was little known about why that is. That's what we set out to examine in this study," Dr. Tzounopoulos said.
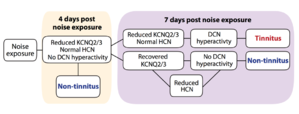
This newest study found that mice that are exposed to loud noise but do not develop tinnitus show a transient reduction in KCNQ2/3 channel activity, which is followed by a recovery of KCNQ2/3 activity and a reduction in hyperpolarization-activated cyclic nucleotide-gated (HCN) channel activity, another channel through which positively charged ions travel in and out of the cell.
The investigators believe a combination of drugs that enhance KCNQ2/3 channel activity and reduce HCN channel activity could promote resilience and reduce susceptibility to tinnitus.
"We have already developed novel activators of KCNQ2/3 channels. The next step, in collaboration with Dr. Peter Wipf, a medicinal chemist from the University of Pittsburgh, is to develop specific blockers of HCN channels," Dr. Tzounopoulos said.
###
Co-authors of the paper are Shuang Li, Ph.D., and Bopanna I. Kalappa, Ph.D., of Pitt's Department of Otolaryngology. The project was funded by the Department of Defense Peer Reviewed Medical Research Program grant PR093405, Joint Warfighter Medical Research Program grant W81XWH-14-1-0117 and by the National Institutes of Health grant R01-DC007905.
 Member
Member

")