Anyone care to take a guess at what happened? Around 35 years old or so.
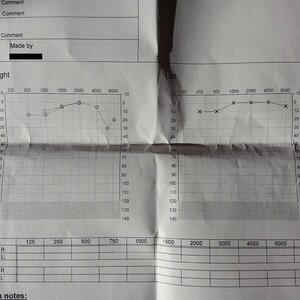
You have hearing loss on your right-hand side, recorded at 6000 Hz. The data point at 6000 Hz probably does not reflect the peak of your hearing loss. That would be a complete fluke. More detailed testing at 250 Hz, or using smaller intervals such as 200 Hz or 100 Hz, would give you a clearer picture of your hearing loss in this range. You might find a bell curve or a skewed bell curve, and the 6000 Hz result would intersect that shape.
Alternatively, you might have a gradual loss of hearing beginning at 5000 Hz and continuing upward. By increasing the resolution of your testing, you will better understand exactly which frequencies are most affected. However, your audiologist probably will not perform this kind of testing.
The result at 8000 Hz on the right side is affected by the decibel hearing level (dB HL) method. This approach adjusts the high and low frequency data points in order to present a smooth and simplified result to the patient. In untreated hearing tests, it is common to see some hearing loss at both low and high frequencies, which is considered normal. The dB HL method tries to flatten the curve for easier interpretation.
Even with this adjustment in place, your audiogram still shows a drop at 8000 Hz, which is significant.
"Our ears do not respond equally to all frequencies. They are most sensitive in the middle range, roughly between 500 and 5000 Hz. Without the dB HL adjustment, a normal audiogram would appear more like an arch than a straight line, which can be more difficult for patients to understand."
The standard intervals used in audiogram testing skip over too much data to accurately show all areas of hearing loss. These common audiograms often have very limited value. A great deal of information between 500 Hz, 1000 Hz, 2000 Hz, 4000 Hz, and 6000 Hz is simply missed. Because testing typically stops at 8000 Hz, even more information in the higher frequencies is left out. That may be exactly where your tinnitus is coming from.
The results at 6000 Hz and 8000 Hz on your right side already suggest a downward trend in your hearing.
Damaged hearing cells do not recover. When they fail to provide enough input, the brain increases its sensitivity, which can lead to tinnitus. In an effort to compensate, nearby intact hearing cells may begin to respond to frequencies they are not naturally meant to detect. If that adaptation is successful, your tinnitus may decrease or even disappear.
However, because your hearing loss seems to progress in the higher ranges, this type of adaptation may not be enough to reduce high-frequency tinnitus.
Since natural sounds are always complex, it is unlikely that your hearing loss exists only within a narrow frequency band, especially if it was caused by noise exposure. A more detailed audiogram with higher frequency resolution would likely reveal moderate hearing loss across additional frequencies.
I have done some personal testing on my own ears and found that complex sounds—which span all frequency bands and are played at the correct intensity—can trigger hyperacusis. The sound duration I tested was 800 milliseconds, which is just under one second. Narrow band sounds did not trigger it. Very short sounds, such as 200 milliseconds, also did not trigger it.
The kind of sound I tested appears to activate all functioning hearing cells until it reaches the range where I have severe hearing loss. At that point, the higher frequencies in the sound are simply not detected by the remaining cells. I suspect that, due to recruitment, a group of somewhat damaged but still active cells is overburdened by the incoming sound, which results in pain.

 Member
Member