Why would the small molecules get deeper into the cochlea for IHCs than for OHCs? I don't see why it would be any different for IHCs.
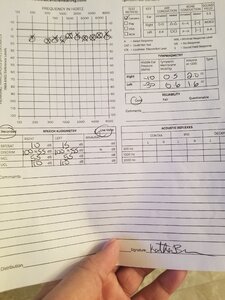
They emphasise clarity in regards to the >8kHz region, because their solution is limited in the sense that it does not get beyond the base of the cochlea. In fact 8kHz may seem like it's beyond halfway the cochlea, but in reality it's still the basal region. If you look at a cochlear diagram you quickly see the compound barely enters the cochlea if it only reaches 8kHz. Their hydrogel will need to improve drastically for it to reach the apex and hence they adjusted objectives and expectations towards intelligibility (clarity), because they attribute clarity to the UHF region. In that sense, without improving the hydrogel, it will look as if this is an absolute success. In my opinion all their clarity statements refer to UHF improvements, both IHC and OHC.
David Luchino only answered the cochlear synaptopathy question in the sense that the hair cells grow and the nerve endings form ribbon synapses and connect to them. It is definitely not a cochlear synaptopathy drug although that was not that explicitly stated, but definitely implied.
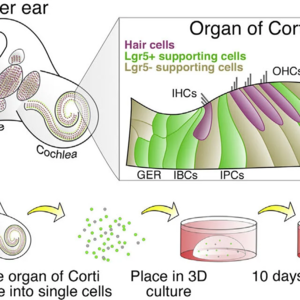
FX-322 regenerates both IHCs and OHCs in the same proportion (although obviously different in absolute numbers). As demonstrated in their 2017 publication.
I would love to have a more in-depth understanding on various aspects of the differences between IHCs and OHCs. I've spent some time studying the difference in functionality in-depth. How they work physiologically and what they're really responsible for when it comes to hearing. It still does not click 100%, but must admit I have not yet spent enough time on it. It is clear though that they are very different. I feel the difference between them is completely overlooked and hardly ever discussed. Even Frequency Therapeutics doesn't touch on this.
Maybe that's why I'm missing what you're speculating about.

 Member
Member