Member
MemberI don't think money would speed up the process. Even the biggest pharma companies with loads of money still have to follow trial procedure and timelines. Drugs just take years to get from concept to market. We're going to have to be patient. ")
I'm curious about nexamerane.
Neramexane
From Wikipedia, the free encyclopedia
Neramexane
Systematic (IUPAC) name
1,3,3,5,5-pentamethylcyclohexanamine
Identifiers
CAS Registry Number 219810-59-0
ATC code None
PubChem CID: 6433106
ChemSpider 4938294
UNII 856DX0KJ84
Chemical data
Formula C11H23N
Molecular mass 169.307 g/mol
SMILES[show]
InChI[show]
(what is this?) (verify)
Neramexane is a drug related to memantine,[1] which acts as an NMDA antagonist[2] and has neuroprotective effects.[3] It is being developed for various possible applications, including treatment of tinnitus,[4][5] Alzheimer's disease,[6] drug addiction[7] and as an analgesic.[8] Animal studies have also suggested antidepressant[9] and nootropic[10] actions, so there are a wide range of potential applications this drug may be used for. It also acts as a nicotinic acetylcholine receptor antagonist.[11]
A clinical trial found that doses of 50mg and above safely improved tinnitus scores over 16 weeks.
https://www.tinnitustalk.com/thread...nitiative-annual-tri-conferences.4/#post-1223So what happened to this drug [Neramexane]!?
reverse this early stage of tinnitus development and prevent longer term tinnitus-related changes in the brain.
so anybody know more? AUT only for early stage or hopefully also for chronic? I thought AUT is for chronic??
This text above was from June 2015. Old/wrong information?
other pharma companies are focused on the NMDA receptors, with AM101, neramexane, gacyclidine and caroverine. I understand that those are good news for new sufferers, since they will have access to a wide variety of drugs intended at this acute stage.

Don't forget 10 % of them had their tinnitus worsened, so in the future many new sufferers will hesitate trying AM101From the Phase II results of AM101, it looks like it substantially improves T "only" in a 62% of the cases.
substantially improves T "only" in a 62% of the cases.
And there will be also people who won't even visit an ENT after a trauma,
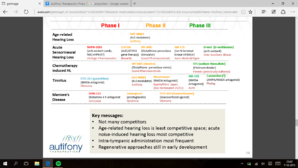
Autifony came back to me.
They have spent a lot of time traveling in the US, getting the Age-Related Hearing Loss trial (CLARITY) underway, and also back home continuing on the momentum of the QUIET-1 trial.
They will however look at the questions as soon as they can and provide answers to what they can.
I'll publish the answers once I receive them.
You don't need to wait.
This link takes you to their own page and you will find all the questions asked, and all the answers that they provided, and that was back on July 16th as well.
")
But only if you've had for between 8 and 12 months!Damn man 2 years,
But only if you've had for between 8 and 12 months!
I saw one doctor who was conducting a trial that he did not expect it to work at all as the T is so complex and everyone's condition is different.
I saw one doctor who was conducting a trial that he did not expect it to work at all as the T is so complex and everyone's condition is different.
Yes, we hear the "T is only considered chronic after one year!" line, but we just don't understand exactly when it moves form the ear to the brain. And it might happen at different times for different people. If AUT works, it will probably have varied responses from users, just like Trobalt. This will be affected by a wide range of things.
Maybe, but the positive results some long-time T sufferers have had from Trobalt shows that it IS possible. Just time for researchers to figure out how!For all we know, it's all in the brain.
The thing about chronicity is that it might be very hard to undo the tinnitus related neuronal network if it has been established for years on end. It becomes part of its ''normal'' function.
My ENT, who "specialized" in T, believed T becomes "chronic" once the potassium channel gates cease to repolarize. Every brain is different, so there is no timeframe. However, if you have T for a month or more from a single event, like noise trauma, there's a good chance it's not going away (although it could). Now, by repolarizing the gates, the T goes away (or is greatly reduced), regardless of how long they've been "stuck". Again, just his theory. Unfortunately, he passed away unexpectedly recently, so he won't get to see the results of Aut
If your ENT knows about potassium channels he is light-years ahead of his peers.
Fingers crossed for aut-0063 or Caroverine or oto-311...
It's likely that the longer the "tinnitus" has been created in the brain, the longer you'd have to take drugs to give your brain to go back to a semi-normal state.My ENT, who "specialized" in T, believed T becomes "chronic" once the potassium channel gates cease to repolarize. Every brain is different, so there is no timeframe. However, if you have T for a month or more from a single event, like noise trauma, there's a good chance it's not going away (although it could). Now, by repolarizing the gates, the T goes away (or is greatly reduced), regardless of how long they've been "stuck". Again, just his theory. Unfortunately, he passed away unexpectedly recently, so he won't get to see the results of Aut
It's likely that the longer the "tinnitus" has been created in the brain, the longer you'd have to take drugs to give your brain to go back to a semi-normal state.
That's ok with me too. One thing I really hope for is that it will help prevent spikes as well. If I could go back to going out in loud places (still wearing earplugs of course) and not have to worry about a spike then this drug would be the holy grail for me.I agree. I feel it'll be a lifetime of meds to keep it surppressed, which is ok with me.
For us I'm assuming this is what we should expect.I agree. I feel it'll be a lifetime of meds to keep it surppressed, which is ok with me.

 Founder
Founder